Demand change to reverse upward pressure on American health care costs
On January 22, 2026, two congressional committees — Energy and Commerce and Ways and Means — grilled the CEOs of America’s largest health insurance companies.
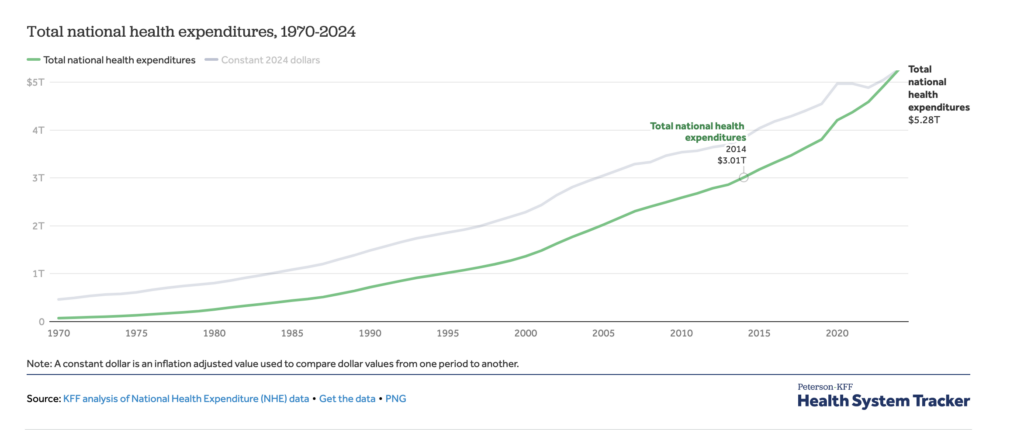
Both committee chairmen began by stating that Americans are getting less health care while paying more and more for it. The United States now spends $5.3 trillion per year, a 77 percent increase since the wildly misnamed Affordable Care Act (Obamacare) took effect in 2014.
Among the hearing’s bright moments was bipartisan agreement on the damaging, inflationary, anti-competitive phenomenon among the largest health insurers of “vertical integration,” the health insurance companies owning numerous subsidiaries that participate in every aspect of providing health care-related products and services.
Representative Alexandria Ocasio-Cortez (D-NY-14) chipped in with a pleasantly surprising free-market slant on the issue, noting for example that CVS Health, known as a pharmacy chain, also owns (1) Aetna, (2) a pharmacy benefit manager, (3) a home health unit, (4) a pharmaceutical manufacturing company and (5) medical clinics. Who would have expected someone usually identified with socialism to call for undoing vertical integration in the health care sector in the name of competition, saying “vertical integration is destroying people’s ability to access care”?
If you’ve been paying attention, you know that getting access to medical care is becoming a serious national problem, even for lawmakers. Representative Greg Murphy (R-NC-03), himself a physician, revealed in a viral video that he had a medication he needs to stay alive denied eight times.
Another physician, Representative John Joyce (R-PA-13) explained a driver of higher premiums by citing the medical loss ratio (MLR), a creation of Obamacare, which requires insurers to spend 85 percent of premium dollars on patient care or quality measures, leaving fifteen percent for profit and administrative salaries.
The arithmetic is straightforward: Fifteen percent of higher and higher numbers means more money available for profit and administrative salaries.
With vertical integration among the insurer, pharmacy benefit manager, pharmacies, clinics, and more, the parent company keeps business “inside the house,” effectively paying more to itself. The process games the MLR feature of Obamacare through self-dealing, which boosts the revenue flowing into the integrated enterprise.
The CEOs who testified before Congress on January 22 know this is the way the incentives are slanted. The parent insurance enterprise can claim they “spent more” on patient care (while paying themselves) and are now positioned to jack up premiums and demand higher taxpayer subsidies under Obamacare. This creates an even larger pie out of which to carve the fifteen percent for profits and salaries. No wonder these CEOs are so handsomely compensated.
It’s perfectly legal, and we tolerate it.
Also discussed on January 22: “Medicare Advantage upcoding,” an overcharging technique used by health insurers… and considered fraudulent by policy shapers as disparate as Senator Elizabeth Warren (D-MA) and Centers for Medicare & Medicaid Services Administrator Mehmet Oz. That upcoding is considered the main driver in $88 billion of waste annually in the Medicare Advantage program.
Despite these issues (and more), American employers continue to retain the services of these gigantic, vertically integrated companies to provide health insurance for employees. (Note: About 61 percent of the workforce has health insurance through their employers.)
Why?
Likely, a lack of understanding, and an inability to see what they are paying.
But an increasingly informed public seems to be making headway with a sluggish Congress.
Exhibit A: In an earlier column, I described the Patients Deserve Price Tags Act that, if passed, would give (1) employers access to the insurance claims they pay for on behalf of their employees, and (2) patients access to itemized bills.
On January 22, Representative Brian Fitzpatrick (R-PA-01) asked the assembled CEOs whether they had any objection to passing that bill.
They did not.
Exhibit B: On January 30, the federal Department of Labor introduced a new rule for self-funded employers that would require pharmacy benefit managers and their related brokers/consultants to divulge detailed information that will make it easier for employers to choose wisely for their employees.
Exhibit C: On February 3, the president signed legislation which included required reforms in the behavior of pharmacy benefit managers. According to Representative Buddy Carter (R-GA-01), a pharmacist, “This is just the start!”
A worthwhile agenda for a reform-minded Congress in 2026 would include:
- Enacting transparency requirements with teeth.
- Making catastrophic insurance (largely illegal since the passage of Obamacare) legal again.
- Expanding tax-advantaged options for meeting medical costs; health savings accounts come to mind.
- Passing the Pharmacists Fight Back Act.
- Breaking up the vertical integration of the big insurers.
The public would do well to understand and push for such reforms, which would create choices and lower costs while curbing the predatory tendencies of corporatized medicine. The public would do well also to assert control over the money they spend on health care. Allowing the government and big corporations to oversee such a huge part of the economy is an open-ended prescription for waste, fraud, and plunder.
Self-funded employers would do well to understand their options and how to make fiscally smarter healthcare choices on behalf of their employees. It’s possible for “little guys” to save money while denying it to the big, vertically integrated health insurers. What a shame that would be!
The congressional committees that interrogated the CEOs on January 22 stated that “other health care leaders” would be called to testify on the root causes of the wild inflation that has rampaged through the health care sector for decades.
Here’s a useful list of witnesses:
- Hospital systems.
- Group purchasing organizations.
- Pharma.
- Distributors of supplies.
- Physicians.
- Pharmacists.
Perhaps hearings to come will be as refreshingly bipartisan and informative as those on January 22.
And we can only hope that the public will learn from them and continue to demand the changes that will finally reverse the relentless upward pressure on the cost of the American health care system.
Marion Mass, M.D., is a practicing pediatrician in Bucks County, a leading member of the Free2Care movement, and a member of The Independence’s advisory board.


